Kidney stones usually comprised of a compound called calcium oxalate, are the result of an accumulation of dissolved minerals on the inner lining of the kidneys. These deposits can grow to the size of a golf ball while maintaining a sharp, crystalline structure.
[wp_ad_camp_1]
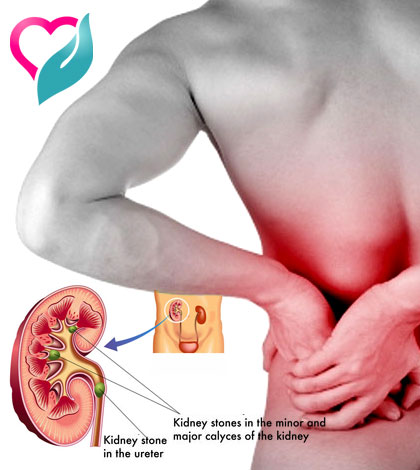
The kidney stones may be small and pass unnoticed out of the urinary tract, but they may also cause extreme pain upon exiting.
Kidney stones that remain inside the body can lead to many conditions, including severe pain and ureter (the tube connecting the kidney and bladder) blockage that obstructs the path urine uses to leave the body.
[wp_ad_camp_4]
What causes kidney stones?
The key process in the development of kidney stones is supersaturation.
- The urine carries salts, including calcium oxalate, uric acid, cystine, or xanthine.
- These salts can become extremely concentrated if there is not enough urine, or if unusually high amounts of crystal-forming salts are present.
- When salt concentration levels reach the point at which they no longer dissolve, these salts form crystals.
Different factors may be involved in either reducing urine amount, or increasing the levels of the salts.
Deficiencies in Protective Factors.
Normally, urine contains substances that may protect against stone formation, including:
- Magnesium
- Citrate
- Pyrophosphate
- Enzymes
These substances:
- Allow salt in the urine to be at higher-than-normal concentrations without forming crystals
- Prevent crystal formation
- Coat the crystals and prevent them from sticking to the surface of kidney tubes
Not having enough of these protective substances can cause stones.
Changes in the Acidity of the Urine.
Changes in the acid balance of the urine can affect stone formation.
- Uric acid and cystine stones mainly form in acidic urine.
- Calcium phosphate and struvite stones increase in alkaline urine.
Medical conditions such as Crohn’s disease, urinary tract infections, renal tubular acidosis, hyperparathyroidism, medullary sponge kidney, and Dent’s disease have been known to lead to kidney stones. It also has been suggested that water fluoridation – the addition of fluoride to drinking water – is responsible for some cases of kidney stones.

[wp_ad_camp_2]
Causes of Calcium Stones
Often, the cause of calcium stones is not known. The condition is then called idiopathic nephrolithiasis. Research suggests that nearly all stones result from problems in the breakdown and absorption of calcium and oxalate. Genetic factors may play a role in about half of these cases. A number of medical conditions and drugs can also affect digestion and intestinal absorption.
Excess Calcium in the Urine (Hypercalciuria).
Hypercalciuria (too much calcium in the urine) is responsible for as much as 70% of calcium-containing stones. A number of conditions may produce hypercalciuria. Many are due to genetic factors, but most cases are due to unknown causes (idiopathic).
The following can lead to hypercalciuria and calcium stones:
- Too much calcium absorption in the intestines: In most of these conditions, genetic factors lead to increased calcium absorption in the intestine.
- Excessive chloride: Chloride has a negative charge, and calcium has a positive one, so they balance each other in the body. Excess chloride may lead to excess calcium.
- Renal calcium leak: In this condition, the does not regulate minerals normally, causing an increase of calcium in the urine.
- Excessive sodium: High urinary levels of sodium result in increased levels of calcium. Certain defects in the kidney tubules transport system, which cause imbalances in sodium and phosphate, can lead to high calcium levels in the urine. A diet high in salt can also produce this effect.
Excess Oxalate in the Urine (Hyperoxaluria).
Oxalate is the most common stone-forming compound. Too much oxalate in the urine is responsible for up to 60% of calcium stones and is a more common cause of stones than too much calcium in the urine.
Hyperoxaluria can be either primary or secondary.
- Primary hyperoxaluria is an inherited disorder in which too much oxalate in the urine is the main problem.
- Secondary hyperoxaluria results from specific conditions that cause high levels of urinary oxalate.
Secondary hyperoxaluria is usually caused by too much dietary oxalates (found in a number of common vegetables, fruits, and grains) or by problems in the body’s breakdown of oxalates. Such defects may be due to various factors:
- Severe vitamin B6 deficiencies (usually due to genetic disorders)
- Deficiencies in Oxalobacter formigenes, an intestinal bacteria that breaks down oxalate
- Short bowel syndrome, a condition that generally results from removal of portions of the small intestines. It causes an inability to properly absorb fat and nutrients. Calcium may bind to the unabsorbed fat instead of the oxalates, which causes a buildup of oxalate
- Androgens (male hormones)
Female hormones (estrogens) actually lower the risk of hyperoxaluria. Estrogen may help prevent the formation of calcium oxalate stones by keeping urine alkaline, and raising protective citrate levels.
Patients who undergo the most common gastric type of bypass surgery, the Roux-en-Y, may be at increased risk for calcium oxalate kidney stones, beginning 6 months after surgery. These patients develop hyperoxaluria, and the condition is common 12 months after surgery.
Excessive Calcium in the Bloodstream (Hypercalcemia).
Hypercalcemia generally occurs when bones break down and release too much calcium into the bloodstream. This is a process called resorption. It can occur from a number of different diseases and events:
- Hyperparathyroidism: Overactive parathyroid glands cause about 5% of calcium stones. People with this disorder have at least a 20% chance of developing kidney stones. Women are more likely to have this disorder than men.
- Immobilization: Lack of movement can lead to kidney stones.
- Renal tubular acidosis: This disorder causes an acidic and alkaline imbalance. Renal tubular acidosis not only increases calcium levels in the bloodstream, but it also reduces protective citrate levels.
Hyperuricosuria is a condition in which there are high levels of uric acid in urine. It occurs in 15 – 20% of people (mostly men) with calcium oxalate stones. Urate, the salt formed from uric acid, creates the center of a crystal (nidus), around which calcium oxalate crystals form and grow. Such stones tend to be severe and recurrent. They appear to be strongly related to a high intake of protein. (Hyperuricosuria also plays a major role in some uric acid stones.)
Low Urine Levels of Citrate (Hypocitraturia). Citrate is the main substance in the body that is responsible for removing excess calcium. It also blocks the process that turns calcium crystals into stones. Low levels of citrate in the urine is a significant risk factor for calcium stones. Hypocitraturia also increases the risk for uric acid stones. This condition most likely contributes to about a third of all kidney stones.
Many conditions can reduce citrate levels. Some causes include:
- Renal tubular acidosis
- Potassium or magnesium deficiency
- Urinary tract infection
- Kidney failure
- Chronic diarrhea
[wp_ad_camp_3]


























